The Headline Number
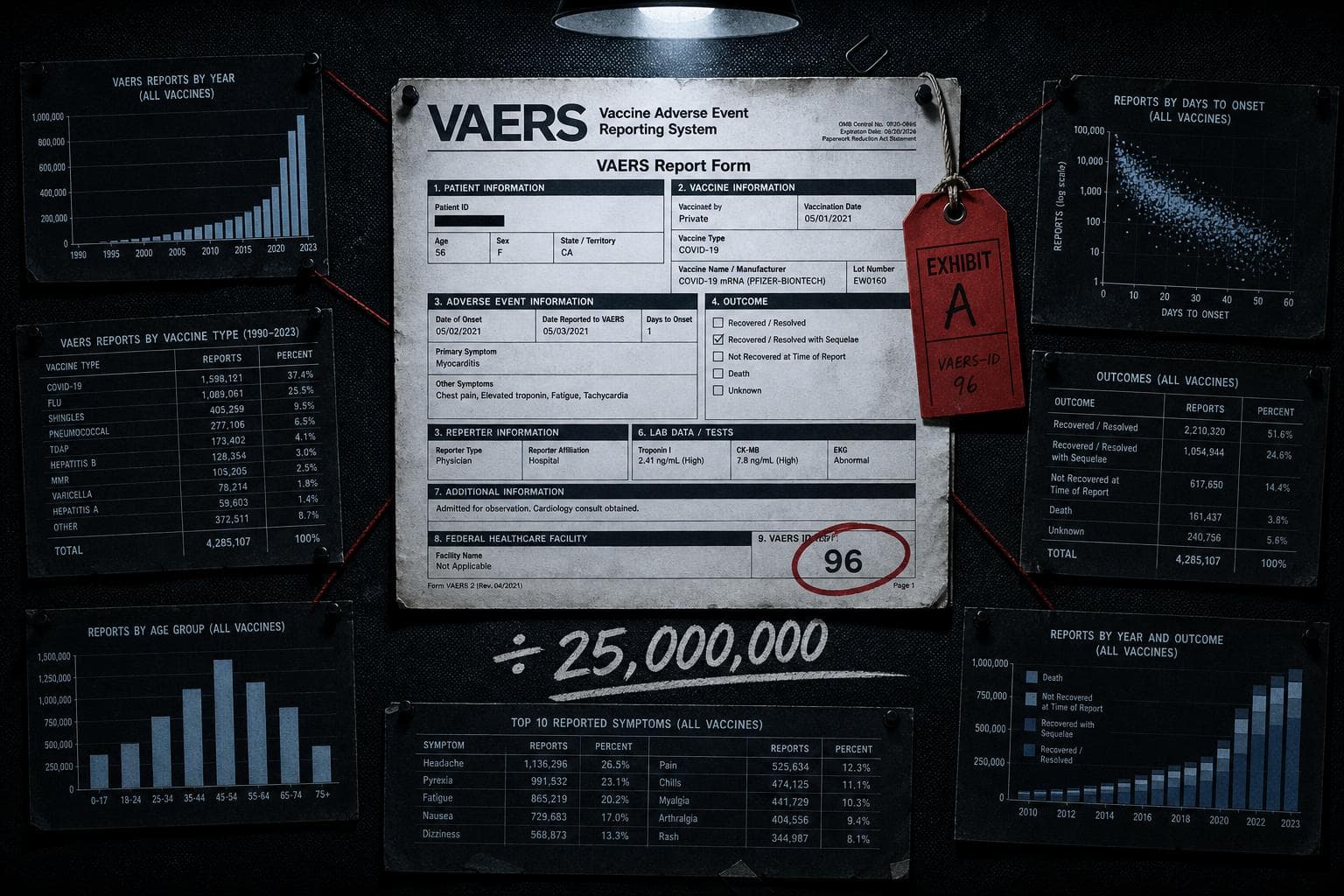
"For the first time, the US FDA will acknowledge that COVID-19 vaccines have killed American children. No fewer than 10 of 96 pediatric deaths reported to VAERS from 2021 to 2024 were caused by COVID-19 vaccination."
— Vinay Prasad, then-director of FDA's Center for Biologics Evaluation and Research, internal memo, November 2025
The Audit
VAERS is a passive surveillance system. That sentence is doing more work than most people realize, so let's slow down on it.
The Vaccine Adverse Event Reporting System accepts reports from anyone — patients, parents, physicians, lawyers, anyone — about health events that occurred after vaccination. It is explicitly not a system for establishing causation. The CDC and FDA have said this clearly and repeatedly since VAERS launched in 1990. The system's own website states that a report to VAERS "generally does not mean that the vaccine(s) caused the adverse event." VAERS is a signal-detection tool: it tells you where to look, not what you found.
Vinay Prasad's November 2025 memo took 96 VAERS reports of pediatric deaths and announced that at least 10 were caused by COVID-19 vaccination. CIDRAP's analysis of the underlying 73-page CBER review — the actual scientific document his memo was supposedly summarizing — found that the memo does not reflect what the career scientists concluded. The report was produced by CBER's Office of Biostatistics and Pharmacovigilance, the office whose job is post-market vaccine safety surveillance. These are not political appointees. This is the team that does this work professionally.
The report does not support what the Prasad memo said.
The Denominator Problem Is Structural, Not Incidental
Here is the number that the memo buried: during the period in question, approximately 25 million children in the United States received COVID-19 vaccines. The VAERS database received 96 reports of pediatric deaths following vaccination across that entire period and population. That is the denominator. Ninety-six reports out of 25 million vaccinated children — before any causation analysis has even begun.
The memo presented 10 as a floor. The underlying science presented it as a ceiling on what could be plausibly attributed after review, and even that characterization requires scrutiny. VAERS reports are not confirmed cases. They are reports. The entire methodological purpose of the subsequent review process is to determine which reports, if any, represent genuine vaccine-caused events rather than coincidental timing.
This is the denominator trick in its most consequential form. You take the numerator (10 deaths attributed), strip away the denominator (25 million vaccinated children, and the baseline rate of childhood deaths from all causes in that age group over three years), and present the raw count as though it constitutes an indictment. It doesn't. It constitutes a starting point for investigation — which is exactly what VAERS is designed to provide.
What the Actual Science Found
The CBER review identified myocarditis as the real signal worth tracking — a known, labeled risk that has appeared on Pfizer-BioNTech and Moderna prescribing information since 2021. The scientists recommended updating the label to address fatal outcomes, because that specific gap existed. That is responsible pharmacovigilance. That is the system working.
But the clinical evidence on vaccine-associated myocarditis in children does not support the alarm the memo implied. The MACiV study, a multicenter analysis of 333 young patients with vaccine-associated myocarditis across 38 US hospitals, reported zero cardiac deaths and zero heart transplants. A Korean national surveillance study of 3.7 million adolescents who received 8.1 million Pfizer-BioNTech doses identified 184 confirmed myocarditis or pericarditis cases — 89.1% mild, with no deaths reported. A French nationwide cohort of 4,635 hospitalized myocarditis patients aged 12 to 49 found no in-hospital deaths among the 558 post-vaccine cases.
These are not small studies. The Korean study covered 3.7 million adolescents. The English national data linked records for 5.1 million children. Canadian active surveillance found that vaccine-proximate myocarditis cases required intensive care in less than 7% of cases, compared with 28% among unvaccinated myocarditis cases — meaning the vaccine-associated cases were, on average, less severe than the naturally occurring ones.
The Prasad memo did not engage with any of this evidence. It cited VAERS counts and called them causation.
The Comparison That Was Never Made
The memo's framing collapses entirely when you ask the question this newsletter exists to ask: compared to what?
COVID-19 infection in children carries its own myocarditis risk — and that risk is substantially higher than the vaccine-associated risk. It also carries the risk of MIS-C (multisystem inflammatory syndrome in children), long COVID, and death. The relevant policy question is not "did any children experience adverse events after vaccination?" The answer to that question is obviously yes, for any medical intervention administered to tens of millions of people. The relevant question is: what is the risk-benefit calculation across the full population, compared to the counterfactual of no vaccination?
The memo did not attempt that comparison. It presented one side of a ledger and called it an accounting.
This is a pattern worth naming precisely because it appears in both directions on vaccine debates. Advocates who dismiss all adverse event reports as noise are making the same methodological error in reverse — ignoring the numerator entirely. The honest position is that VAERS signals require investigation, that investigation requires comparing rates to baselines, and that the baseline here includes the risks of the disease the vaccine prevents. The CBER career scientists understood this. The memo that summarized their work did not reflect it.
Verdict: Misleading. The 10-deaths figure is drawn from a passive surveillance system that explicitly does not establish causation, presented without the denominator of 25 million vaccinated children, without comparison to baseline pediatric death rates, and without the clinical evidence from multiple large-scale studies that found zero vaccine-associated pediatric cardiac deaths. The underlying scientific review does not support the memo's framing.
The Denominator Trick Has a Political Sibling
While the FDA memo was manufacturing a numerator problem, a different kind of statistical malpractice was running in parallel in Washington.
FactCheck.org reported that HHS Secretary Robert F. Kennedy Jr. told a congressional hearing in April that the FDA approved two oncology drugs "in record time — one in 45 days" and that "the closest before that was 310 days." The 310-day figure is the average new drug application review time for all drugs in 2025, per remarks from then-FDA Commissioner Marty Makary. The two fast approvals were for new indications for previously approved drugs — not new molecular entities requiring full safety reviews.
Dr. Aaron Kesselheim of Harvard Medical School told FactCheck.org that comparing these approvals to the all-drug average is like "comparing apples and gorillas." New indications for existing drugs are structurally easier to review. The comparison is not wrong because the numbers are fabricated. It's wrong because the denominators are incompatible — you cannot benchmark a subset against the average of a much larger, more complex population and call it a speed record.
The FDA's own Commissioner's National Priority Voucher program, announced in June 2025, targets review times of one to two months for qualifying drugs. Seven drugs have completed review through the program as of FactCheck.org's reporting. Whether that represents a systemic improvement in approval speed — or a selection effect where easier-to-review drugs are being prioritized — cannot be determined from seven cases. Kesselheim said it's "a little bit soon to evaluate" the overall impact, given the "relatively small" number of drugs reviewed entirely under the new administration.
That is what intellectual honesty sounds like. It is not a common sound in congressional hearings.
By the Numbers
44.8 — The University of Michigan Consumer Sentiment Index reading for May 2026, described by Material Truths as an all-time low in the continuous series, below the 1980 stagflation trough and the 2008 financial crisis. The reframe: sentiment is a leading indicator of spending behavior, not a lagging measure of economic conditions — when it diverges this sharply from headline GDP (reported at 2.0% growth in Q1 2026), the question isn't which number is right, it's which one predicts what happens next.
18 — The number displayed when hovering over Spain on HantavirusMap.com, which viral social media posts claimed showed confirmed hantavirus cases. The actual confirmed case count in Spain linked to the MV Hondius cruise ship outbreak: two. The map's creator built it to aggregate news articles and public alerts, not confirmed infections — a distinction his own disclaimer stated clearly, which did not stop the screenshots from spreading with voiceovers claiming otherwise.
82% — President Trump's estimate of Iran's missiles that are "gone," cited during a Cabinet meeting this week, per CNN's fact-check. The reframe: CNN reported in April, citing three sources familiar with US intelligence, that roughly half of Iran's missile launchers were still intact — and that Iran's military is reconstituting faster than initially estimated. The gap between 82% degraded and 50% degraded is not a rounding error; it's the difference between a defeated adversary and an active one.
The thread connecting all three of this week's numbers is the same one it always is: the headline figure was chosen because it was available, not because it was the right one. The VAERS count was available. The all-drug average was available. The map's alert count was available. None of them answered the question they were being used to answer. The denominator — the baseline, the comparison, the full population — was inconvenient, so it didn't make the memo.
Watch for the CBER review's full public release and whether any congressional oversight hearing examines the gap between the Prasad memo's claims and what the career scientists actually wrote. That document is now an exhibit in a Senate letter. It will not stay quiet.


