For decades, the advice was so routine it barely registered as advice. Older adult? Take your calcium and vitamin D. Keep your bones strong. Stay on your feet. It was the kind of recommendation that came from doctors, pharmacists, and well-meaning relatives with equal confidence, backed by a logic that seemed almost too obvious to question: vitamin D helps your body absorb calcium, calcium builds bone, therefore supplements should prevent fractures. Case closed.
Except the case, it turns out, was never really closed. A large systematic review and meta-analysis published in The BMJ has now assembled the most comprehensive picture yet of what the clinical trial evidence actually shows — and the answer is considerably less reassuring than the supplement aisle would suggest.
153,000 People, 69 Trials, One Uncomfortable Finding
The review, led by Olivier Massé and colleagues at a Montreal research center, analyzed 69 randomized controlled trials involving 153,902 participants. These weren't fringe studies or industry-funded outliers — the team used established bias assessment tools and rated most of the evidence as moderate to high certainty. The participants skewed toward exactly the population most likely to be taking these supplements: a median age of 71, about 87% living independently in the community, and 73% not classified as high risk for fractures or falls.
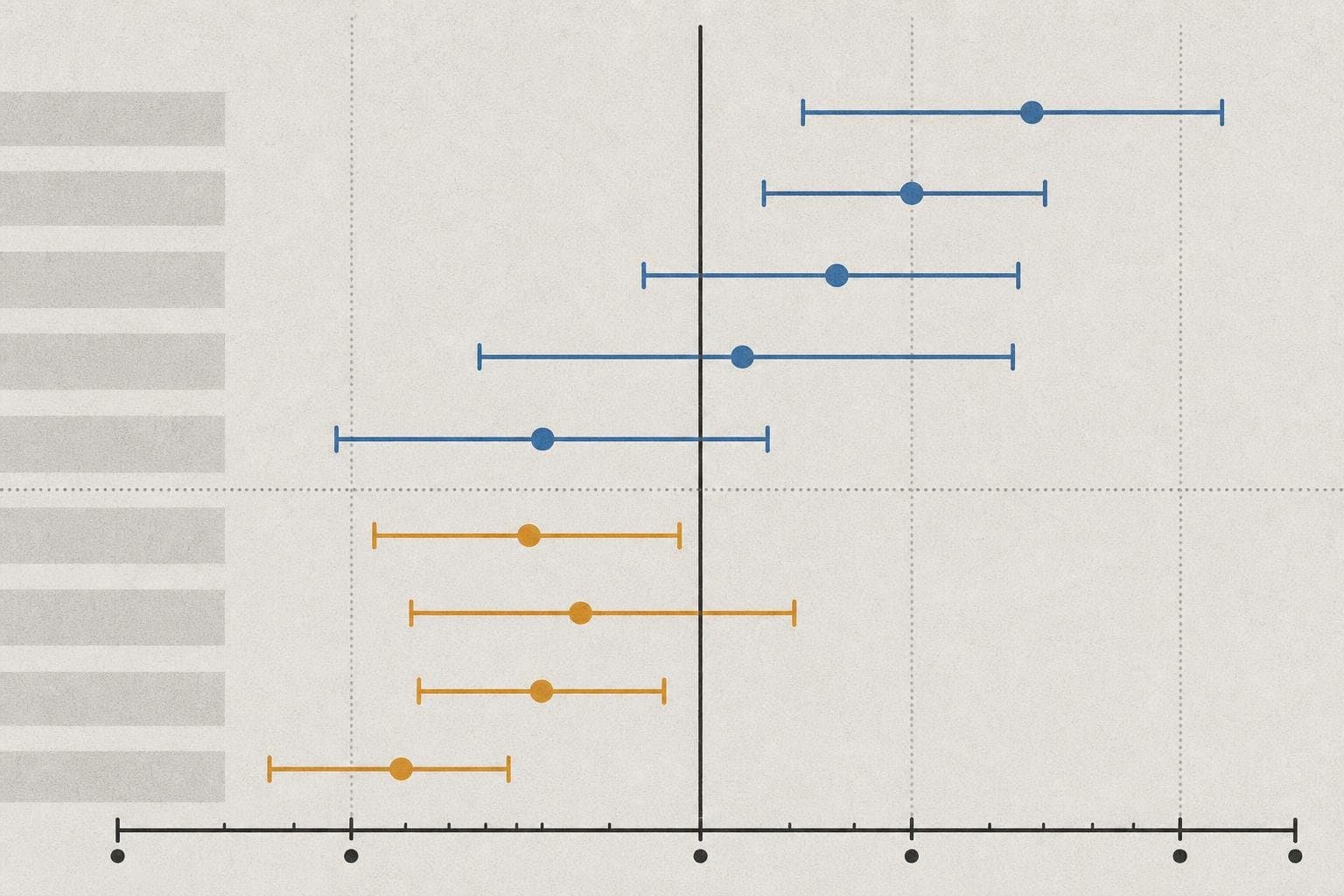
The results, broken down:
- Vitamin D alone: Across 36 trials and over 92,000 participants, no difference in fracture risk compared to placebo. High-certainty evidence. No effect on falls either.
- Calcium alone: Across 11 trials, no meaningful difference in fracture risk. Moderate-certainty evidence.
- Combined calcium and vitamin D: A small statistical signal — a relative risk reduction of about 9% for any fracture — but the researchers concluded this did not meet their pre-specified threshold for clinical meaningfulness. The absolute risk reduction simply wasn't large enough to matter in practice.
The conclusion from the authors was direct: these findings "do not support routine supplementation with calcium, vitamin D or combined supplementation to prevent fractures or falls."
The Gap Between Mechanism and Outcome
Here's what makes this finding genuinely interesting rather than just deflating: the underlying biology isn't wrong. Vitamin D does promote calcium absorption in the gut and is needed for bone mineralization. Deficiency causes real problems — rickets in children, osteomalacia in adults. The mechanism that justified decades of supplementation recommendations is real.
The problem is the leap from "this nutrient matters for bone health" to "therefore giving supplements to people who aren't severely deficient will prevent fractures." That leap turns out to be much harder to justify than the mechanism alone implies. Observational studies associated low vitamin D levels with low bone density and falls — but as anyone who's spent time reading nutrition research knows, association and intervention are very different things. When you actually randomize people to take supplements and follow them for years, the effect largely disappears.
This is a pattern worth recognizing. It's the same gap that has undermined antioxidant supplements, fish oil for heart disease, and a long list of other interventions that looked compelling in observational data and then failed in trials. The mechanism is real; the supplement doesn't reliably deliver the outcome.
What Actually Works
The BMJ editorial accompanying the review pointed toward what the evidence does support: balance and resistance exercise, and multicomponent interventions combining exercise with hazard assessment or education tailored to individual risk. These are less convenient than a pill, which probably explains why they're less universally recommended.
For people already taking prescription medications for osteoporosis, or those with documented severe deficiency, the picture may be different — the review's authors noted the evidence was more limited for high-risk patients and those in residential care, so this isn't a blanket dismissal of vitamin D's clinical role. Treating deficiency is not the same as supplementing healthy people into better outcomes.
But for the millions of generally healthy older adults taking calcium and vitamin D as routine prevention — a habit that one estimate put at roughly $2 billion annually in the U.S. and EU — this review is a serious challenge to the default recommendation. The intuition behind it was reasonable. The evidence, accumulated across 153,000 people, doesn't support it.
The supplements aren't dangerous. They're just probably not doing what most people think they're doing. And at some point, "probably not harmful" is a pretty thin justification for a recommendation that's been handed out with the confidence of established fact.


