Your three-year-old has eaten the same four foods for six weeks. You've tried hiding vegetables in pasta sauce. You've tried the "one bite" rule. You've tried making the broccoli look like a tiny tree. None of it worked, and now you're Googling whether this is a phase or a problem.
Here's the disorienting thing: the research suggests the question itself is historically novel.
Picky Eating Wasn't Always the Default
Helen Zoe Veit, a Michigan State University associate professor who spent roughly 14 years researching children's food culture, argues that the modern conception of children as naturally selective eaters is a surprisingly recent development. In the 19th century, children typically ate the same meals as adults — seasonal vegetables, organ meats, fermented foods — without a separate "kids' menu" framework. "Over and over, I kept bumping into older sources describing children enjoying foods they weren't supposed to like," Veit told Newsweek.
Her explanation centers on structural changes, not biology. Pre-industrial children arrived at meals genuinely hungry — fewer snacks, more physical activity, longer gaps between eating. They also participated in food production: tending gardens, feeding animals, helping cook. That investment changed their relationship to what appeared on the table. And critically, there were no easy alternatives. If you refused dinner, there was no backup option waiting in the refrigerator.
The 20th century reversed all of this. Packaged snacks reduced pre-meal hunger. Milk was promoted as a near-complete food and consumed in quantities that dampened appetite. And the cultural shift toward child-centered eating — the idea that children have distinct, legitimate preferences that adults should accommodate — created the feedback loop we now call picky eating.
This matters for intervention, because it reframes the problem. If picky eating is partly a structural and environmental phenomenon, then the most effective responses are probably structural and environmental too.
When "Picky" Becomes a Clinical Signal
Before getting to what works, it's worth being precise about when to worry. Most toddler food selectivity is developmentally ordinary — neophobia (fear of new foods) peaks between ages two and six and is well-documented across cultures. The clinical threshold is different.
Research on children with neurodevelopmental disorders is instructive here, because it shows what severe food selectivity looks like at its extreme. Children with autism spectrum disorder and ADHD show feeding difficulties at substantially higher rates than typically developing peers, often driven by sensory processing differences rather than preference or stubbornness. The distinction matters: a child whose nervous system registers certain textures as genuinely overwhelming is not the same as a child who has learned that refusing dinner produces a preferred alternative.
Avela Health's clinical framing puts it plainly: "It's really important to remember that this is physiological. They aren't just being difficult." For autistic children especially, sensory input — smell, texture, temperature, the visual appearance of a plate — can register as extreme rather than merely unpleasant, triggering a genuine nervous system response that shuts down appetite.
The practical signal for parents: if food selectivity is severe enough to affect growth, if the accepted food list is shrinking rather than stable, or if mealtimes involve significant distress rather than ordinary negotiation, that warrants a conversation with a pediatrician. A cross-sectional study from northern Vietnam found an association between picky eating and stunting in children aged 12–35 months — though that study's context (ethnic minority children in a mountainous region with different baseline nutritional access) limits how directly it translates to well-resourced settings. The association is worth noting; the magnitude isn't straightforwardly generalizable.
What the Intervention Evidence Actually Shows
The honest answer is that the intervention research on typical toddler picky eating is thinner than parenting culture implies. What exists points in a consistent direction, even if the effect sizes are modest.
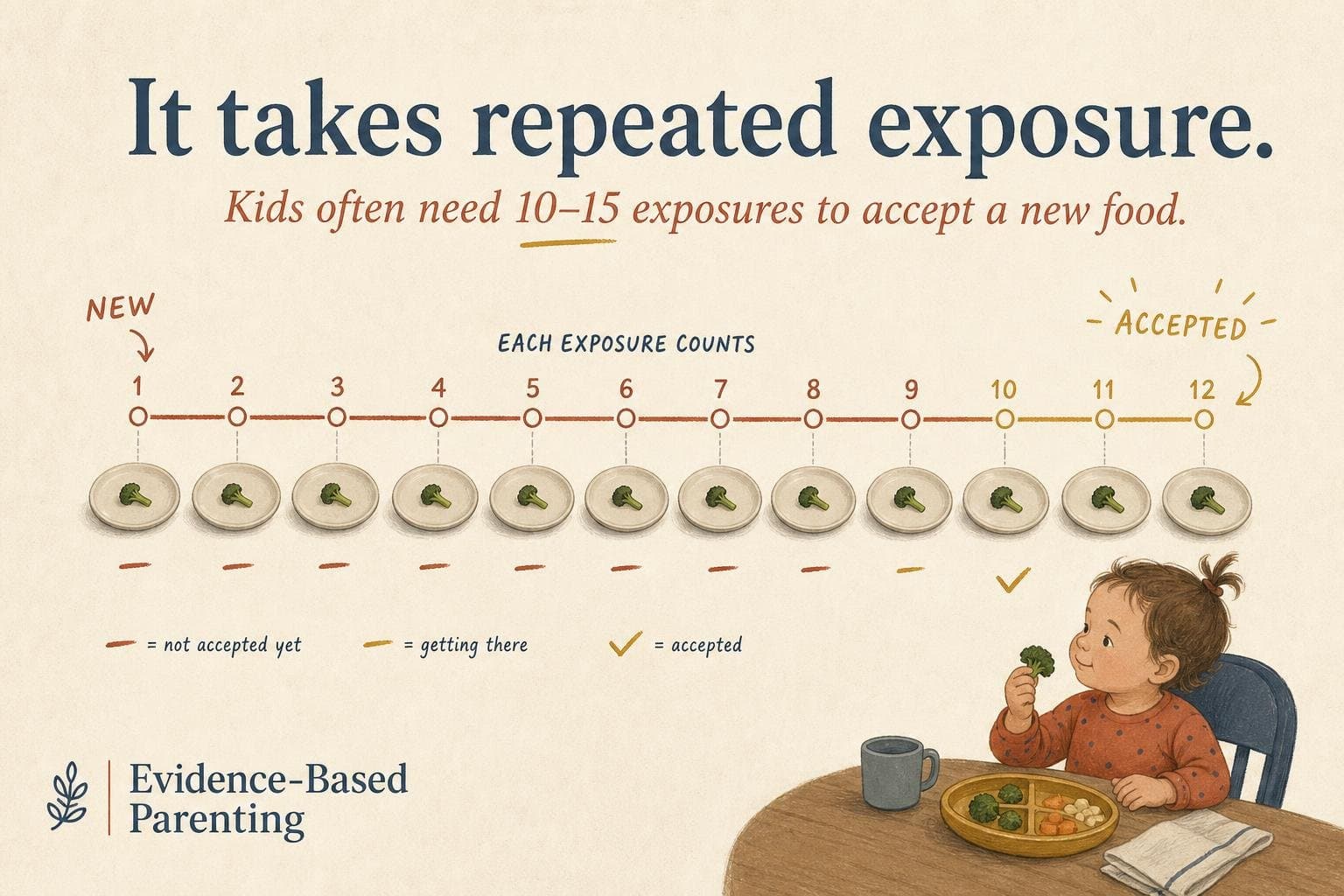
Repeated exposure works — but it takes more repetitions than most parents attempt. The research consensus is that children may need somewhere between 10 and 15 exposures to an unfamiliar food before accepting it, and "exposure" means the food appearing on the plate, not necessarily being eaten. Parents who give up after three or four rejections are stopping before the intervention has had a chance to function.
Pressure backfires. Coercive feeding — the "one more bite" rule, rewards contingent on eating, emotional reactions to refusal — is consistently associated with worse outcomes in the literature. The mechanism Veit's historical analysis suggests is relevant here: children who feel controlled around food lose the internal appetite cues that make eating self-regulating.
Structure helps more than most parents expect. The meal timing and regularity meta-analysis published in the International Journal of Obesity — which synthesized 30 observational studies involving over 100,000 children — found that skipping main meals significantly increased obesity risk, with consistent findings across breakfast, lunch, and dinner. The mechanism isn't fully established, but the pattern supports what Veit's historical argument implies: children who arrive at meals with genuine hunger are more likely to eat what's served.
The practical synthesis: serve the food, don't force it, keep meals regular, minimize snacks close to mealtimes, and expect the process to take months rather than days. That's not a satisfying protocol. But it's what the evidence supports — and it's meaningfully different from the anxiety-driven accommodation that most parenting advice quietly encourages.
If your child's accepted food list is stable or slowly expanding, you're probably watching a normal developmental process unfold on its own timeline. If it's contracting, that's the signal to escalate.


